
When most people think of the word “desert,” they likely picture a dry, cracked, barren landscape far from civilization. But when it comes to pharmacy deserts, you’re as likely to find one in a major city like Chicago or Los Angeles, as you would in a more rural setting.
/Dry%20landscape%20in%20sepia%20shades%20with%20cracks%20on%20the%20ground.jpeg?width=1000&height=750&name=Dry%20landscape%20in%20sepia%20shades%20with%20cracks%20on%20the%20ground.jpeg)
What are pharmacy deserts?
The origin of the term goes back to 2014, when Dima M. Qato, PharmD, MPH, PhD, then a faculty member at the University of Illinois, Chicago, coined the term “pharmacy desert” in a 2014 article in Health Affairs. She and the article’s other authors employed the concept of “food deserts” – already in use by the U.S. Department of Agriculture – to describe a census tract where residents did not have ready access to a supermarket or large grocery store. The agency defined low access as more than one mile from a supermarket or a large grocery store in an urban area, or more than 10 miles in a rural setting.
Put simply, a “pharmacy desert” is any area with subpar access to prescription medications. Pharmacy access may lag for a variety of reasons: low income, insurance status, high prices, inadequate transportation, long distances, or a combination of those factors.
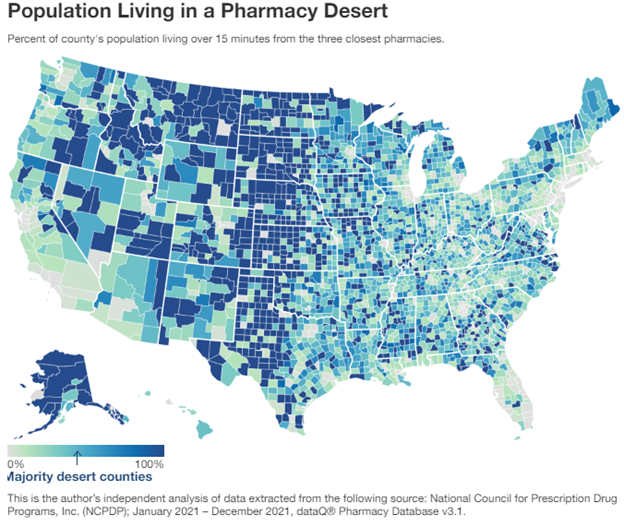
According to a recent study by GoodRx Research, over 40% of counties are pharmacy deserts, where most people have to drive more than 15 minutes to reach nearby pharmacies. The company recently published a white paper that reveals how healthcare infrastructure, or lack thereof, shapes access to healthcare.
New Mapping Tool May Shed Light
A week ago, the National Community Pharmacists Association (NCPA) and University of Southern California (USC) jointly announced the creation of a new interactive mapping tool that could promote health equity by identifying pharmacy deserts in the United States.
“Pharmacy access is critical not only to Americans who depend on them for lifesaving medications but also for the rollout of public health initiatives such as vaccinations, contraceptives and HIV prevention,” says Qato, who is now USC Associate Professor of Pharmacy and Spatial Sciences and Senior Fellow with the USC Leonard D. Schaeffer Center for Health Policy and Economics. Qato is co-director for the USC-NCPA Pharmacy Access Initiative's Pharmacy Shortage Area mapping project, along with NCPA’s Ronna Hauser, PharmD, senior vice president of policy and pharmacy affairs, who serves as co-director.
The new mapping tool defines pharmacy shortage areas as neighborhoods in which the nearest pharmacy is more than 1 mile away for urban, 2 miles away for suburban or 10 miles away for rural neighborhoods. The distance is a half mile for low-income neighborhoods, where most households don't own a car. These defined areas are in line with recent published, peer-reviewed research.
“Traveling a mile to get your prescription medications may be convenient for people that own a car,” says Qato. “But traveling a mile, or even half a mile, may be difficult for people who live in low-income neighborhoods and don’t drive, particularly older adults who rely on walking or public transportation.”
Black and Latino neighborhoods in the 30 most populous U.S. cities had fewer pharmacies than white or diverse neighborhoods, according to USC researchers. Pharmacies are vital points of care for essential health services, and pharmacy deserts affect nearly 15 million people. Nationwide, nearly 70% of Americans take at least one Rx drug, a number that is likely to increase as the U.S. population ages. Plus, older patients are among the most likely to have pharmacy access problems.
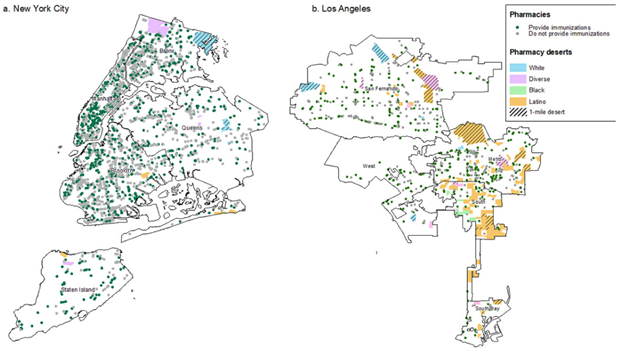
One in three neighborhoods throughout the 30 largest US cities are pharmacy deserts, according to Public Health Post research. Nearly 40% of segregated Black and Latino neighborhoods are deserts, compared to one quarter of White neighborhoods.
“Millions of Americans may live within what appears to be a modest distance to a pharmacy, but they don’t have a car or access to public transportation,” says B. Douglas Hoey, CEO of NCPA. “That severely limits their access to pharmacies in the area.”
The tool’s interactive maps will generate real-time information for national, state, and local policy officials, healthcare academics, industry leaders, and others to identify communities lacking in pharmacy access at the neighborhood level. Better data on the proliferation of pharmacy deserts could help policymakers and industry leaders and, ultimately, underserved communities.
PBMs, Pharmacy Chains Worsening the Problem?
“Reimbursement is the main issue in pharmacy closures that contribute to pharmacy deserts,” says NCPA’s Hauser. “States are making it more obvious that they want to help pharmacies succeed and continue to stay open in these underserved areas.”
The NCPA is fighting for improved pharmacy access at both the federal and state levels. Arkansas, California, Louisiana, Oregon and Virginia have passed laws requiring better pharmacy access, improved dispensing fees, stronger PBM oversight, and other patient- and pharmacist-positive changes in their Medicaid programs, Hauser says.
Meanwhile, Ohio has taken on OptumRx for overcharging the state’s workers compensation program. The state’s auditor found that pharmacy benefits managers (PBMs) had extracted $244 million from the Ohio managed care Medicaid program using spread pricing.
“CVS Caremark is noteworthy because it has a very obviously competing retail arm that benefits every time a competing pharmacy closes,” says Anthony Ciaccia, who served as director of government and public affairs for the Ohio Pharmacists Association, and now leads 46brooklyn Research, a drug supply chain consultancy. “But I can’t name a PBM that doesn’t have its own mail order or specialty pharmacy that profits from reduced retail competition. Community pharmacy closures are a benefit to the companies that price them out of the market by cutting reimbursement.”
Ciaccia noted that Ohio has seen a surge in pharmacy deserts as unprofitable rural pharmacies close. In early 2019, the Ritzman regional pharmacy chain, sold to CVS. The mega-chain closed 16 of those drugstores, creating “instant pharmacy deserts,” says Ciaccia.
Independent Pharmacies Part of the Solution?
While big chain pharmacies point to mail order as a solution, research has found that patients overwhelmingly refer face-to-face pharmacy services to mail order. A J.D. Power study on pharmacy customer satisfaction indicates that more thorough pharmacist discussions produce higher customer satisfaction and customers are happiest with independent pharmacies.
Telepharmacy, which got new life during the pandemic, may be a large part of the solution to pharmacy deserts. Some independent pharmacists are expanding their existing community practices with telepharmacies, either independently or in cooperation with medical clinics or retailers such as grocery and hardware stores, Federally Qualified Health Centers, hospitals, and other provider groups. So, pharmacy deserts could present tremendous opportunities, in both rural and urban settings.
.svg)
.png)



.png)
