RxSafe was pleased to sponsor How Specialty Pharmacies are Revolutionizing Patient Compliance.
Hosted by Todd Eury, publisher of the Pharmacy Podcast Network, the webinar included guests:
• Brad Livingstone, PharmD, Owner, Sound Specialty Pharmacy
• Matt Gilbert, VP of Strategic Accounts, RxSafe
“Pharmacy runs through this guy's veins,” says Eury, speaking of Brad Livingstone. “He's been expanding his pharmacy businesses from compounding to community pharmacy, specialty, mixed long-term care, and the services that have been critical to the communities where he operates.”
Below is a recap of the webinar highlights, questions and answers. Some of the answers have been edited for brevity and clarity.
Click on the image above to watch the full webinar
Q1. Would you tell our listeners a little bit about your background?
Brad Livingstone: Sure. I’m a Washington State University grad. Class of ’96, go Cougars! Shortly thereafter I became manager of a long strokes here in Olympia, Washington, and then well, I left pharmacy for a little while to pursue a music career, and then I came back and started my own temping agency. So I had the opportunity to work in 70 or 80 pharmacies in the State of Washington and had a staff, a pharmacist in tech. So I got a chance to see a lot of things that were done well, and a lot of things that weren't done well.
At that time I had started a family with some young kids. I wanted to be closer to home, so I transitioned from that to an ownership role with some partners who operated a retail pharmacy, at that time called Northwest Specialty Pharmacy, and then we purchased a compounding-only pharmacy. So that was sort of my baby, from 2009 to 2017, which was compounding and nutrition. When I left my partnership, in 2017, I opened up my current pharmacy in 2018 and been here ever since.
We're a specialty pharmacy by name, but we do a lot of things: long term care (LTC); we have some specialty channels; and we are actually are located on the behavioral health resources campus here in Olympia. So we partner with our community really closely. And I also served on some boards over the years, and have just tried to be involved as much as I can.
Q2. Well, I appreciate you being here. You and I know how critical those partnerships are, expanding what we do, and how much RxSafe has participated in building content for community pharmacy owners. And they’ve started really expanding into long term care, and now specialty pharmacy.
So my next question is for Matt. You and I have talked offline many times about expanding a business. I really want to start out with you just as a table set. What are the primary factors contributing to the anticipated 8% annual growth rate of the specialty pharmacy sector through 2025?
Matt Gilbert: A few of the key drivers are: One or more drugs are being classified and paid for by third parties and PBMs as specialty drugs. The PBMs are driving that business back to themselves, which is at least partially true. But that growth and the year-to-year pricing strategies that all these drug manufacturers are using, that's contributing to the growth rate. So the more that enter the market, they've got a long runway before the brand-name drugs go generic. The price keeps going up and up and up, and more people end up on them. It's just a market that's been exploding more than any other over the last, say, 10 years.
Q3. Brad, how do you see it, from the trenches? We want specialty pharmacies to be as successful as possible in this business, so I’d like to get your perspective on this explosive growth over the next 10 years.
Brad Livingstone: Frankly, I'm surprised it's only 8%. Because if I take what we sell that's classified by CMS anyway, as a specialty drug the threshold is $830 for a 30-day supply of a particular ingredient, which is classified as a specialty pharmaceutical. We sell a lot of those, and the pricing strategies are the primary driver. I think, for a number that low, we used to see a 6% annual increase. And now we see a 4% biannual increase in most of those medications. So I'm surprised. I think it's going to be higher than that -- honestly, higher than 8% -- because we're going to have a lot more products coming into the market driven by data and driven by pharmacogenomics.
Q4. How do you envision the landscape of the pharmacy industry evolving over the next decade? You just brought up pharmacogenomics, the role of the pharmacist meshing compounding, long-term care, and specialty pharmacy. Give our listeners a little bit of your vision of the evolving landscape.
Brad Livingstone: I think with so much data out there and the ability now to aggregate that and analyze it, it's going to be easier to look at someone's individual profile, as far as what their DNA says they will or will not handle, and everybody's their own little chemistry set, right? So if you if you can condense that for people and develop individualized therapy for them, then that's something that gets me excited. It's something that I think would be super beneficial for obviously patients, but also professionally in terms of [pharmacist] satisfaction, it would be great for that. The key is: how do we protect some of that, so that it actually supports a business model as well? There's a lot that goes into it. But I think that over the next 10-15 years is going to be an explosion of AI and people who are able to get individualized therapy based on their genomics.
.jpg?width=818&height=387&name=RxSafe-PPN-SpecialtyRx%20(2).jpg)
Q5. As the industry shifts toward more personalized medication, to complex and rare disease states, how do you think pharmacies can be better prepared to adapt to this change?
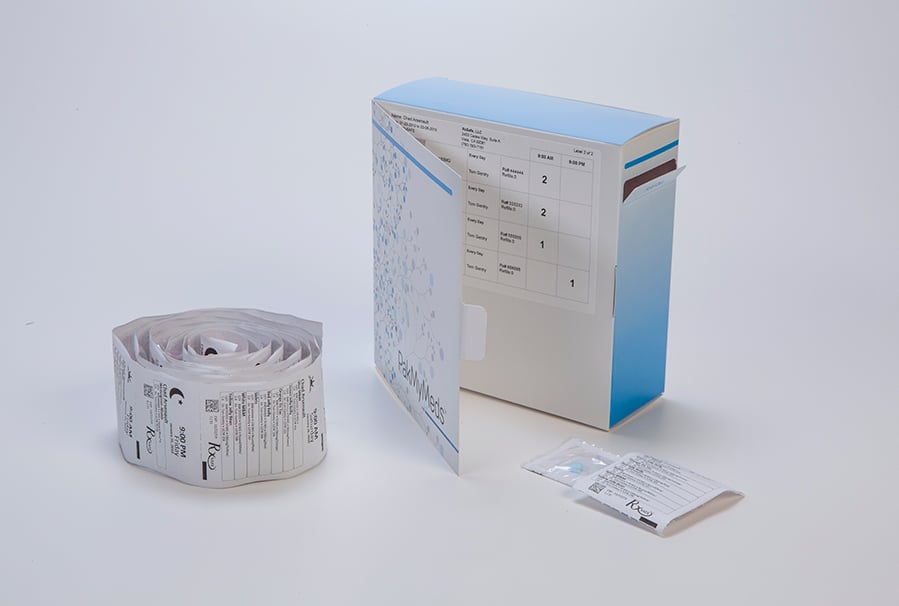
Matt Gilbert: From an RxSafe perspective, we want to be able to produce, pouches through our RapidPakRx technology to keep patients adherent, and that's not exclusive to just their medications. It’s targeted vitamins, nutraceuticals, targeted OTC therapies that may or may not be paid for by their PBM, but that the pharmacy is recommending for nutrient depletion reasons. We want to take a holistic approach to it instead of saying, “All right. Well, we want to make sure you're adhering on your on your strict Rx items.” That is not our game.
Brad Livingstone: I just echo a lot of Matt's thoughts on personalized medicine. When I graduated from pharmacy school, you learn a lot about the commercially available drugs. What you don't really learn a lot about was just basic care of the human body. I had a mentor, Randy Mentzer, who graciously sold me his compounding pharmacy, who was a clinical nutritionist, and I learned so much from him. He was an amazing man. Unfortunately, he's no longer with us, but the difference that he was able to make in our small community. The guy had fans like I've never seen in pharmacy, ever.
He made me a true believer. What he made me see was the bias, toward certain data that was paid for with big money, rather than talking to people and finding out how they're doing and spending the time, like you say, in the trenches, working with people and refining their therapies. I think that pharmacies could really benefit by getting their staff trained up on some of these integrated approaches. When you're treating these complex disease states, that means looking at the root of some of the problems, not treating just the symptoms.
It's my belief, and I'm sure the belief of a lot of people, that inflammation is the root of all evil. So it's addressing those underlying conditions. And naturopaths and physicians, there's a role for everybody in this. Then and then you can really put a powerful and individualized package together for a person, and you can watch them progress. And that's the exciting part about it for me. But you gotta get people trained up. You have to spend a little bit of money and get them trained and send them to the right places to get that training.
Q6. How do you see the role of the pharmacist changing, and specialty pharmacists in particular, and how to educate themselves to prepare?
Brad Livingstone: I think for me and for us as a pharmacy team. We find the causes that our community cares about. One of the big problems that we have locally is homelessness and drug use and opioid use disorder. We've got a big fentanyl problem now. And so we've developed relationships over the years with certain doctors in the area who've been working on various pathways towards treating this population of people. And it's that kind of relationship for me that has dictated which direction we were going right now. And as we grow, maybe we can add additional complex disease states. But you can't be everything to everyone, not when you're my size. So you have to pick your battles, and really know how to communicate with the clients and the caregivers, and connect them with other stakeholders in the community who provide resources.
For example: someone who's in Al-Anon. Well, there's Al-Anon. But then there's also another part of Al-Anon that provides support to the people who care about those going through recovery and addiction. So there are all these disparate resources in our community are coming together. So we're intimately involved at this point in making sure that we understand the needs of our community as it evolves, because it just does. I mean, when we opened 5 years ago there wasn't any fentanyl, and now treatment strategies have changed dramatically for that particular disorder based on the introduction of fentanyl.
Q7. I think of the word ‘competition’ when you're talking, and I know that the hospital systems are very focused on specialty pharmacy. Matt, when I think of the conversations that you have with customers in different territories throughout the country, who want to get deeper into specialty, what are the essential knowledge or skills that you may talk to a community pharmacy about to really, effectively navigate and tap into this specialty pharmacy boom?
Matt Gilbert: Yeah. Just about every pharmacist I talk to tells me they're not a salesperson, and they're not a marketing person, and my response is always, “You are by default. It's either you or it's never going to happen.” So specifically what my team does at RxSafe and the business transformation department when somebody buys a piece of our technology, we actually fly out there and go on site with them for a couple of days and hold their hand and bring them to drug detox centers, prisons, assisted living facilities, skilled nursing, home health agencies… I have visited a 3-bed facility in the backwoods of Kentucky, and I've been to 2,000 bed, 3,000 bed, 4,000 bed SNFs. It's just crazy, [the size of] these campuses.
But one thing that came to mind when Brad was talking about some of the opioid dependents: we took one of our partner pharmacies down in Georgia and went to a drug detox center. And it was really interesting getting inside the walls and getting the mentality of the facility. It's a state-run facility where they don't have a lot of resources. They have low adherence rates. They have technicians or nurse’s aides that are going in and administering medication. And the average length of stay was only 3-and-a-half days. So basically, they get them off of whatever they're on, and send them on their way.
But what our pharmacy did down there was, go in there with pouch packaging as the lead, but getting into a cash-based system. So there's no PBM involvement. There's no doctors’ fees. So you’re creating a cash payment system where not only you're getting the patient taken care of while they're in detox, but it's a long term relationship. We're going to bring this patient into the family of the pharmacy and make sure they're taken care of afterwards, when they're on their own. So little things like that add up. Independent pharmacy is the biggest chain that there is. There's 20,000 of us, and I say ‘us’ because I was a part of that community for 15 years, running two stores in Connecticut. But that's all I deal with, and we want to make all of you -- the Brad Livingstones of the world -- successful. So we'll do it any way we can. We want to make sure everybody's successful.
Q8. So, Brad, how are you managing customization? Because you made comments about your size, and I don't necessarily think that's a barrier to care for patients. I think it's just your reach into what networks you're part of, and what access you have to different payers and things like that. But in your community, you're extremely important, because you're the go-to organization that people are coming to for answers. So talk about customized prescriptions and specialty pharmacy, and enhancing that patient compliance and adherence. Safety is always on the mind of the pharmacist. So how does that customization and custom care in specialty pharmacies enhance medication adherence?
Brad Livingstone: I'll just use an example of our behavioral health business. We do a lot of long-acting, antipsychotic injectables and we'll administer them also for physicians that don't want to do that on-site. So the big problem is always when these folks go inpatient, and then they're discharged, they get lost before they show up for their first community appointment with a provider. We help manage that part, so that they don't get lost. They do not get forgotten about, and the RapidPakRx is one way that we're able to send that out [compliance packaging] with the client. Make it easy. So when they're discharged, make it as easy as possible for them to stay compliant with their medications, and sometimes you have a provider who will give that long-acting injectable before they're discharged, which is great, very helpful, but sometimes not. And so we also want to be that resource for the providers to give our professional opinion about where this client is, and ask what they would best benefit from. And so the RapidPakRx is a great tool that we have that makes us competitive in our market, or any in any market. It's scalable, and it's very configurable. It really helps us grow our business, and it really keeps us from losing business, more importantly.
Matt Gilbert: I think when you talk about that, too, Brad, going into a hospital that doesn't have its own outpatient pharmacy, and doing a similar program, whether it's ‘meds to beds’ or something else, being able to say to them, “Hey, we're going to manage that whole discharge medication process for you, and we're going to reduce your admission rates.” I mean, what better selling point is there for an independent pharmacy going to a hospital than saying that? I can't think of one.
Q9. Just to follow up, Brad, I wanted to pull more of that information out. You mentioned behavioral health, but what other disease states are you seeing in terms of the ability and the opportunity to build customized programs to keep people adherent?
Brad Livingstone: Right now we're focused on behavioral health and the opioid use disorders. And the thing about the two of them is, it's ‘the chicken or the egg.’ They either have a mental health disorder that led to drug abuse, or vice versa. So those two for us are what's driving us currently. I'm celiac [laughs]. So I have a spot in my heart for people who are celiac. I wish we could come up with a cure for that. That'd be great. But managing celiac disease, that is another place where I feel like I can make a difference in in people's lives. And there's not a ton of specialty meds out there for it, but you could help manage it with supplements and avoidance.
Q10. I'm thinking of medication adherence issues that are specific to specialty pharmacy. Let’s say you do a follow-up with a patient. And all of a sudden, their payment source changes, and that really could become very disruptive to treatment. So what type of medication adherence issues are you facing in specialty pharmacy, and how are you addressing those?
Brad Livingstone: I know we could be billing an injectable for them, and then they change insurance, and all of a sudden it's prior auth, or it's got to be done out of another pharmacy somewhere. We typically don't just take ‘no’ as a no, we're a little thorn-in-the-side most of the time, or if we don't get the answer that we're looking for, and that can benefit the patient, from the insurance company, we will involve the provider. Because of our relationships we have with the providers, they go to bat for us and for the clients, because they know that this is in the best interest of someone who is dependent on this adherence for staying on track. And so we've been successful most of the time doing that. But it's kind of like, “Don't take no for an answer.” And, you're going to get NOs. But when you do that, when you don't just give up on your community, on your people that you take care of, you've got to advocate for them. You have to advocate for yourself. That's how you get it done.
Brad Livingstone: Unfortunately, the biggest challenge for us is that we're roughly 70% Medicaid [patient population], and so it's is hard when you're we have probably 6 or 7 MCOs with their own PBMs that are Medicaid contracted in Washington state, so not all of them pay well and on brand names in particular. So we're talking about specialty meds predominantly, brand name medications that you have a very thin margin on. The pain threshold, it's up there, you know. We're doing the right thing as a community benefit for our folks, and we just continue to hope that doing that will bring in other lines of business, that will help offset that. Really, it's hard to ask a community pharmacy our size, that does mostly Medicaid clients, to continue to dispense at a loss, and a significant loss. And so ultimately, you know we don't want our decisions about this kind of treatment or that kind of treatment to be directed by PBMs. That is the old fight, right? And unfortunately, sometimes that is a driver.
Q11. Matt, I know because of how many pharmacists and pharmacy owners that you're talking to that this ‘limited distribution’ issue comes up. There's the examples that I was talking to Brad about patient training and compliance management and clinical data reporting. What's coming up when you're out in the field, when you're talking with community pharmacies that have now expanded into specialty? What are the drivers of success that you're helping them to foresee so they can be better prepared for it?
Matt Gilbert: The biggest thing that we find from the field -- and I talk to probably 5,000 pharmacy owners in a year, maybe more -- the biggest thing that they're dealing with from a specialty perspective is: how do we effectively manage this treatment? How do we keep them adherent? And how do I monitor that without it costing me an arm and a leg, and then getting a negative reimbursement on top of it sometimes?
So the thing that RxSafe has really delved headfirst into, over the last 6 months, is setting up an RTM program that is very, very dumbed down. You know, it's the most basic tracking mechanism that we can do out of one of our dispensing boxes. But what that does is, it frees up the pharmacist from calling every week or every other week. I know real-time if my patient took that medication at 8 AM, or noon, or whatever time it was, and it alerts me as the pharmacist saying, “Hey, this is somebody that missed their dose or missed two doses, and we wanted to check in on them to keep them adherent.” A lot of the technology that's out there is very sophisticated, and it's got huge dispenser devices. It's cumbersome. It costs a lot of money, which is cost-prohibitive for the pharmacy as well as the patient.
And so we went out and made some partnerships and some solutions that are going to be rolling out in the next few months with us. And it uses our technology, so if you use our pouch packaging, you've got access to this whole new world and a whole new billing mechanism for certain disease states on top of that. So you can not only provide a better quality of care to a patient, you're actually going to get reimbursed a lot for it.
Those are things that we're constantly hearing and taking feedback from prospects and customers and going to pharmacy conferences. And that's why we do 40 tradeshows a year, because we learn so much from everybody. Every single conference I go to, we pull a new idea out of that, and that's why we do them. It's not just to sell equipment. We want to be a true partner with everybody and take their feedback and improve our products through that.
Q12. Brad, what comes into play with follow-up, not just with the patient, but also communications with the payer, and communications with the provider, the physician. How are you communicating to physicians who are handing off their patients to a specific specialty pharmacy that has technology and this packaging to assure adherence?
Brad Livingstone: Yeah, we basically just walk them through the process. I mean I'll use an example of a Sublocade network, where there’s a very defined RMS (Risk Evaluation and Mitigation Strategy)process. And it's not the doctor's office there, because now they don't have to have the special DEA number in order to be able to prescribe they basically just prescribe it, and they want it delivered. But there are all these guidelines that we have to follow as a pharmacy, so to help them understand from our perspective what it takes to make it go smoothly requires that we're talking with every single provider in that clinic about the requirements and making sure that we provide them not only with REMS guidelines, but maybe any sort of specifics about how we do it or when we're going to be able to deliver those products out to their clinic, what our expectations are, what their expectations are, and then communicating when it's actually administered, so that we're making sure that we're following up in that in the timeframe. In Sublocade, it’s around 30 days, the time that we're following up. There's a subsequent appointment that they that they're scheduling, so that we can have the product in stock, and just make sure that that process goes as smoothly as possible. But it's not something you can really do, If you just think of yourself as being a traditional retail pharmacy or anything like that. You have to kinda bake all those services into your business model and figure out how you're going to train your staff to maintain that contact, and streamline it.
Q13. Matt, let’s talk about innovation. What major shifts in innovation should we anticipate in specialty pharmacy over the next decade?
Matt Gilbert: I think I think the biggest thing is going to be bringing adherence packaging to the masses, and that's not exclusive to pouch packaging. There are a lot of people out there where Blister Card is their preference. Different homes and facilities where they've had a nursing staff that's been on there, and these could be single or multi-dose the Dispill or Medicine on Times of the world. But that's why, we actually created a machine called the rapid card. That is the same front-end process as the RapidPakRx, same footprint, and the output just goes out in cards, and it uses any type of card stock; we don't sell cards or anything like that. But specifically for this purpose, we knew there's going to be facilities out there and patients out there where they want to stick with one modality. That's been growing exponentially on both the pouch and the card for the last 5 or so years, and with more and more people aging and staying in place at home, you're going to have more and more people taking specialty medicine at home and not dispense in a facility. So we want to make sure that we have something that can accommodate any type of modality where they could need packaging.
Q14. So Brad, what have you seen in innovation that we can anticipate in specialty pharmacy tied to promoting adherence and compliance?
Brad Livingstone: I'm just excited by what Matt's talking about. I have seen the RapidCardRx, that card producing version of the of the RapidPakRx, and that I think for me, that is likely to be the next step, because you're exactly right. I mean, there are some big fans of strip packaging, and there are some who just don't like it. It's all about meeting the clients where they're at and sort of anticipating their needs, but also using technology to keep our expenses from getting out of control, as things get more complex and harder to manage. So I'm excited to see where things are going.
Q15. When we were at the NASP Conference, we ran into a company called Pharma Soul. They do personalized texting that's attached to a database and library, and the AI knows what stage of treatment the patients are based on the NDC that's selected, and then it will send them personalized text that makes the patient feel like it was a text from a human being, saying something like, “Hey, how are you feeling today?” And the patients might respond, “Not so well,” and the text or the AI might reply, “On a scale from 1-10, how nauseated are you feeling?” because it knows that nausea is a component of that stage of treatment. What I think is going to help compliance, just from being out there and listening and watching and interviewing, is personalization for each of the patients or what they're going through. And I'm thinking, well, how do we do that when, Brad, you have hundreds, if not thousands, of patients? If I took every patient that was impacted by RxSafe technology, it would be in the millions. I don't even know if you have a number for that, Matt, but it's enormous, right? And I'm thinking, how can we utilize better ongoing communication to ensure that adherence is taking place, without burdening the individual pharmacy that would have to make hundreds, if not thousands of calls. So, Matt, that's kind of one for you. What are you thinking from an innovation perspective?
Matt Gilbert: From an integration perspective, I get calls or emails or LinkedIn messages every week from different vendors and different people that want to be partners, or maybe a pharmacist who moonlights as an engineer and says, “Hey, I came up with this cool device; what do you think?” For example, earlier this week, I got a call from a guy, and he said, “I've got this dispenser that I've made. I don't have anybody using it right now. But here's the use case for it.” And it was if you scanned in one of the bar codes on our pouch, and then, right before that, it would alert either audibly or with a light on it, for somebody who had hearing issues going on. It's time to take your medication, you scan in the pouch, and then it records and tracks that. But as a follow-up to that, he said, “I've also got this other use case where I've got this summer camp for these children that are going through all sorts of treatments, cancer treatments. And I got a question from one of the parents, and they asked if it would be possible, if we go forward with you, and we find a partner pharmacy, and we do the pouch packaging? Could you write a note on every pouch that says, ‘Hey, Kevin, hang in there, do this, do that each day, you're killing it.’ And I said, “Yeah, we can do that. We have free text fields. You could put blank pouches in there. We can write anything we want.” And he was just blown away by that. Now, is that a true medical necessity? No. But is that going to improve that patient's life? Hell, yeah. So there are just really cool things that we get to talk about every week, and there's so many great ideas out there from the technology sector.
Q16. It's the ability to customize that communication. I think of the box that some RxSafe customers will put their strip packaging into, and on that box is personalization opportunities and marketing opportunities and explanations of that treatment. And I also think of packaging and storage and the importance of temperature control, and all of that is much more easy to manage, than just handing somebody a vial of tablets. But expand upon that, Matt, because you see that you see that every day.
Matt Gilbert: Yeah, and one of the big benefits is we can fit a ton of medication in one single pouch. So instead of doing 2 or 3 med passes, or 2 or 3 tear-offs, you're doing one. It's making it as easy for the patient as possible. You're taking a very dry, sterile experience that used be, you know, “Here's 20 vials. Go take one of each or 2 of each.” And instead you’re putting it into a pouch with a customized font on it, and the branding from the pharmacy on there, and maybe a message on there for the patient. So you’re going from that sterile environment for the patient of, “This is a task I have to do,” but you’re reducing that by probably 20x, time-wise, and making it something that they actually enjoy doing.
Q17. This is a good question for you, Brad, because of the experience of very specific NCDs that you're managing, and that is the manufacturer's sensitivity around who is allowed to distribute a specific medication based on the need for REMS reporting or packaging or cold storage, or the time that the patient gets onto therapy as quickly as possible. Talk to me about your perspective, because there are independent community pharmacy owners that are wondering how to get into specialty pharmacy from the beginning, or how to get deeper into specialty pharmacy with regard to the relationships around manufacturers. How are you managing that?
Brad Livingstone: We’ve kind of found, I guess we could say almost a back door into the specialty channels by making ourselves a strong and almost indispensable community partner with, particularly with the Bupe Clinic here in Olympia. We're at 800 or a thousand clients who are struggling with opioid use disorder. And so really, the providers who were using us through the clinic, were also using national specialty pharmacies to get product. But it just wasn't working for various reasons. So out of necessity to reach this client base where they're at, it was kind of, the start of discussions through MHA our buying group, about becoming part of the network. And so we've been doing it now about 6 or 7 months, and it's really starting to gain some traction there, and we’re seeing some positive results as from that. So it's exciting, it really is.
Q18. So, Matt. You get this question I’m sure, on a regular basis from community pharmacies that have a good reputation with patient, doctors, manufacturers and payers, but they say to you, Matt: from your experience, how do I get deeper into specialty? How do I expand my specialty business? What answers do you have?
Matt Gilbert: Well, I think piggybacking off what Brad said earlier, he’s a smaller fish in the pond, but that doesn't mean he's not a fish in the pond. You know, networking locally is the single biggest thing, regardless of what denomination of pharmacy it is, that you can do. And building out those prescriber networks and saying, “Here, we're going to offer you a higher level of service for your patients. We're going to make it as painless as possible. Here's my direct cell phone number.”
I tell that to a lot of our pharmacists who have our RapidPakRx and RapidCardRx machines. Go to a prescriber and tell them here's my personal cell phone number. If you need something, call me. And see what kind of impact that makes. And business goes through the roof. Every big box store that's in town, they would never do that.
I think the biggest thing that pharmacists can do is believe in themselves as a partner versus a vendor. You don't want to be the dispenser, the guy that everybody envisions. You know, the pharmacists sitting on the bench, counting by fives. That is not the case at all. The pharmacist is doing everything they can to keep the pharmacy afloat, and coming up with all these new ideas and branching out into different networks and getting special contracts for these different drugs. So there's a lot of different levers they can pull. But I think the biggest one is believing in themselves as a partner and going out and partnering with the different physician networks.
Brad Livingstone: Yeah, don't allow yourself to be so siloed that you're just pharmacy. I mean, if you're having an issue with the laws, even the laws of your state, guess what? You can partner with some physicians, and you can find some people to actually get laws made or changed, if it makes sense for patient safety and adherence or outcomes. When you're talking about that sort of thing, you have lawmakers and they just don't know what they don't know. Many are well-informed. Many aren't. If there's something that needs to be changed, you gotta let somebody know, and do something about it.
Q19. This whole ecosystem is so important, but sometimes that ecosystem is disrupted by those profit elements of our big, huge, conglomerate PBM-driven pharmacies that are really not looking at the individual. Everyone on this webinar right now is focused on the individual and the patient need, and the patient compliance and the patient follow-up. So how can specialty pharmacies ensure a patient-centered approach while still maintaining profit and scalability?
Matt Gilbert: From an RxSafe perspective, we get pretty creative. So whether it's no money down, or no payments for 6 months, we get pretty creative with the financing, and we also customize each of our solutions to that pharmacy. So we have the ability to scale up the RapidPakRx and RapidCardRx from a 20-cartridge to a 30- to a 40-cartridge. Some people buy multiple units. Some people want an enterprise server where they're dispensing or sending orders from 3, 4, 5, 6, 10, different stores, and we can accommodate that. So the nuance to each store is totally different. No two pharmacies are the same. No two pharmacy owners are the same. So whether it's customizing the machine, the software, the back-end marketing support that they need, customized boxes, etc., we really want to take a holistic approach and find what fits for that particular pharmacy and helps them take it to that next level, whether that next level is just getting into specialty or just getting into LTC or just getting into combo shop, or just opening a retail pharmacy. We've got people that worked on the bench for a chain store for 20 years and said, “I'm burnt, man. I'm going to open a store, but I love your machine. I want to get it in there. How can we do that?” We help them do that. So we're here to help.
Q20. That's awesome. I appreciate that. That comes through your entire staff, too. I've talked to several people on the RxSafe staff. It always reaches out and finds the answer. And, by the way, some of the best answers that have come from RxSafe have actually come from the Brad Livingstones of the world, which is their customer base and the information base. And that's why I want to come back to you, Brad, and just get your viewpoint on profitability and scalability as a pharmacy owner. That's a challenge. And sometimes you lose a couple of patients, maybe because of a contract change and you have to make that up. What's your strategy around keeping patients compliant. That's key. That's the safety that I'm talking about, keeping them on the treatment. But let's talk about profitability and scalability from your perspective.
Brad Livingstone: Well, obviously, profitability is always a huge factor for us. I mean, if you're going into the specialty world where you're doing a lot of brand name stuff, you've got to have a certain pain tolerance for low margins. But also keep in mind that it's a percentage game, and if you're selling a larger dollar amount, you can sometimes get away with the smaller percentage, and not overload yourself with work. I appreciate RxSafe, and that they're always listening to people like me. So I appreciate that. And I always feel like they want to know what could help us, and that they're actually working to solve our problems as community pharmacists, not just looking to sell or force-feed an industry what they come up with. So I appreciate that. So I'm always looking to see what they have as the next great thing coming out and making sure it fits with what we're doing here. There are so many advantages to having a small footprint, super configurable, scalable machine, where I don't have to increase my inventory. All the advantages that small businesses really have to pay attention to. Because I think many who have been doing what we've been doing for a long time know that it's a shell game. Like next year, where's the money? Is it under this shell? Is it under that shell? Is it going to come from rebates? Is it going to come from a different payer mix? What's it going to look like? So those are those are challenges that you just have to rise up and meet every year. But you've gotta just have a thick skin and know that doing the right thing for your patients ultimately will pay off.
And if you look at this in the future as, “I'm going to help you, the individual,” there's an opportunity there for you to feel good about making some money charging cash for a product or a service that's not offered by someone else, that's going improve a patient’s health or outcomes. It just makes life more enjoyable, not only for them, but for you as a pharmacist. I mean, otherwise, you get stuck in a pharmacy just counting pills. That's not for me.
Q21. Yes, and that's an element of pharmacy where we have to be honest with each other as an industry. We have chain community pharmacists that are going through a tremendous amount of burnout. The majority of them are just beautiful people that want to help other people. They're intelligent. They want to be more clinically driven. And that kind of ties back to the whole theme today, which is understanding the compliance barriers. And one of those barriers is making it simple for patients to stay on their medications and not make it a complex thing where you're worried about how many vials of medication that you're on. Matt has taught me that putting in supplements inside these packs, where we know there might be a deficiency in something happening in this person's life. And, you know, put in a vitamin B-12 complex or add something in there that can help them.
Brad Livingstone: Yeah, and communicating that to the prescriber, whether it's patient-driven, or whether you'd want to talk to the prescriber directly about some of the things that they don't know they could be prescribing, even the advantage here in our state, if they go ahead and write a prescription for a supplement, then at least you save on the tax. It's advantageous for everybody, and then we can keep track of it. The physician can keep track of it, and the patient is getting the benefit. So win-win for everybody.
Matt Gilbert. Yeah, and especially getting to the end of the year, too, I'll leave everybody with one final thought. It's a tax season coming up. So IRS Section 179 gives you advanced depreciation on any capital equipment purchases. I know Brad used that. So you save a ton of money, put it back in his pocket instead of paying the IRS, which is always a good thing, but you've got to get that equipment installed in the year that you claim it. So right now we're bumping up to booking out towards the end of the year, as far as installs go, but we can still accommodate a few more. So if anybody's had a good year, and wants to explore our technology, use Section 179. Put some more cash in your pocket.
Todd Eury: That's awesome. We appreciate RxSafe and your partnership with the Pharmacy Podcast Network. And I like these discussions, because they're educational. And I want to thank you, Brad, for being our special guest today.
.svg)




.png)